


 Overview
Overview
On April 27, 2016, the Centers of Medicare & Medicaid Services (CMS) released proposed updates and rules to the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA). In 2015, MACRA was originally implemented to establish a new way to reimburse physicians and increase the use of information technologies, as well as move health care organizations away from fee-for-service and towards pay-for-performance. With the recent changes, the proposed rules are meant to improve the method by which provider Medicare payments are tied to cost and quality of care, thus hopefully accelerating the desired shift to value-based payment (VBP) and higher quality care through the expansion of pay-for-performance incentives. It repealed Medicare’s sustainable growth (SGR) formula, expanded the Children’s Health Insurance Program (CHIP) and established the Merit-based Incentive Payment System (MIPS) and Alternative Payment Models (APM).
CMS has developed various types of innovative programs for providers to select that allow them to choose the best-fit option to incentivize the movement to VBP and establish the MIPS and APMs. However, the array of options under MIPS and APM contribute to fragmentation and confusion in the measurement of quality and value. The newly proposed Quality Payment Program streamlines and unifies the various MIPS and advanced APM programs to become a single payment adjustment to help clinicians transition to VBP. Introducing the Quality Payment Program and its associated changes to MACRA will streamline and integrate healthcare delivery, increase Electronic Medical Record (EHR) use and adoption, as well as increase provider participation in MIPS and Advanced APMs. In this article, we will explore the proposed changes to MACRA’s MIPS and APMs with the implementation of the Quality Payment Program.
Proposed Updates to MIPS
Currently under MIPS, measurement is done through a selection of programs, including the Physician Quality Reporting System, the Value Modifier Program and the Medicare EHR Incentive Program. Under the proposed rule, the three programs will be unified under MIPS to improve the relevance and depth of Medicare’s value and quality-based payments, leading to an overhaul in the framework in which CMS conducts performance measurement and determines physician payments.
As described in the diagram below, the new framework of performance measurement will consist of four categories (Cost, Quality, Clinical Practice Improvement Activities and Advancing Care Information), each with updated criteria. CMS will begin measuring performance for participating providers through MIPS in 2017, with payments based on those measures beginning in 2019. The first performance period for new incentives is to begin by 2017 with the first payment period in 2019.
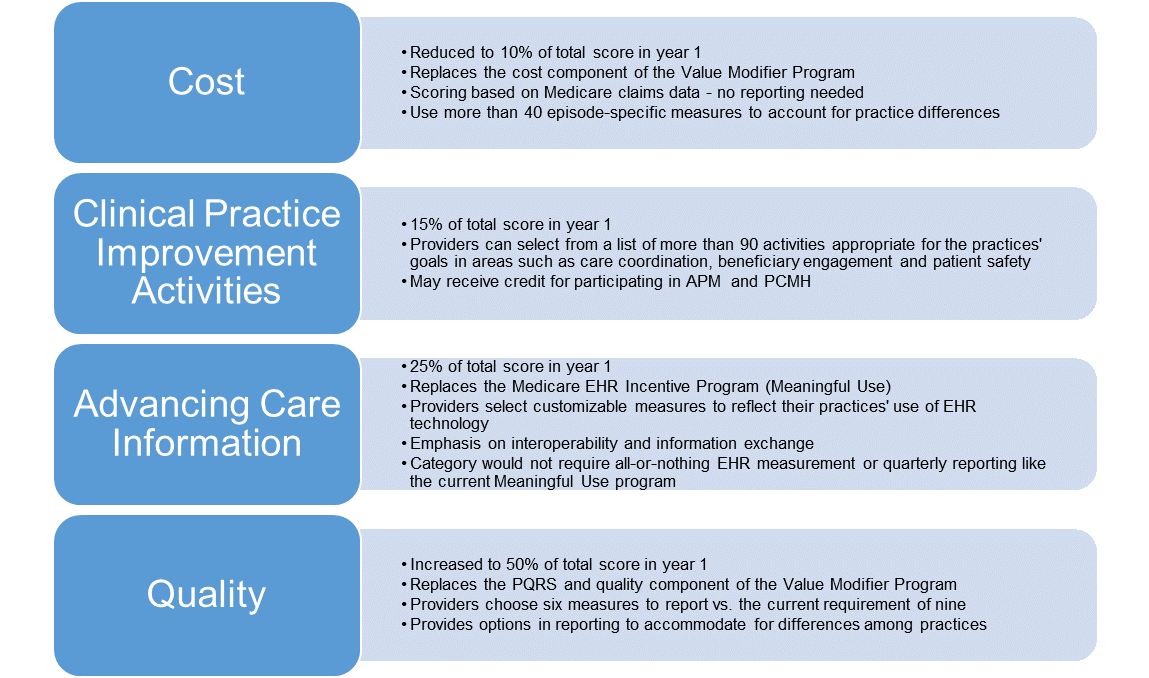
The listed performance measures for the four categories reflects increased flexibility due to negative Medicare provider feedback in 2015. This improved list enables providers to select the ones most appropriate to the type of care they provide. As providers begin to implement improvements and achieve their merit based incentives, they can further complement their services by joining Advanced APMs.
Proposed Updates for Advanced APMs
In regards to Advanced APMs, the proposed rule provides various incentives for providers to participate in these models. One of the various incentives is that they would be exempt from MIPS payment adjustments and qualify for a 5% Medicare Part B Incentive Payment for years 2019 – 2024.
MACRA envisions two types of payment models qualifying for the APM track: models requiring providers to take on financial risk and models involving medical homes. The new rule consolidates the CMS Innovation Center Models, Shared Savings Program options, and statutorily-required demonstrations to be listed under Advanced APMs. The list of models that would qualify under the terms of the proposed rule as Advanced APMs includes the following: Comprehensive ESRD Care Model (Large Dialysis Organization arrangement), Comprehensive Primary Care Plus (CPC+), Medicare Shared Savings Program – Track 2, Medicare Shared Savings Program – Track 3, Next Generation ACO Models, and Oncology Care Model Two-Sided Risk Arrangement.
Originally, CMS disallowed Medicare Shared Savings Plans (MSSP) ACOs from participating in advance payments for establishing medical homes. However, CMS now recognizes that by allowing physicians to participate in both CPC+ and ACOs, this could eliminate the ACO disincentive and boost both initiatives.
The proposed rule also defines the APM modification process and qualification requirements, qualifications necessary for incentive payments, and the establishment of the Physician-Focused Payment Technical Advisory Committee. CMS requires that Advanced APMs meet specific requirements and standards. As these models are still improving and growing, CMS continues to modify the list to assist in Advanced APM qualification, which will be updated yearly. Expansion of this list of CMS approved models provides more opportunities for Advanced APM leaders and providers to push their entities and the health care industry towards VBP.
Looking Forward
As the health care industry moves towards VBP, it is important to understand how providers will be affected by these proposed MACRA changes regarding incentive reimbursement, quality reporting and financials.
Effectively determining and distributing physician payments through performance measurement generates various challenges for physician organizations, such as defining a fair way to assign fees or penalties and promoting efficient use of resources and high quality care. The perceived fairness of the distribution of these savings needs to be accepted by the providers in order to ensure continued support of the model. Providers should consider the cost of resources and technology to implement and adapt to the chosen CMS program, as well as the amount of risk-adjustment based on each of their respective populations. If all goes well for the providers, they can make up what they have put into the organization via reimbursement and incentive payments. However, large amounts of time, money, and resources are necessary for the provider to achieve the required goals. Smaller practices will be less likely to take part in these improvements to the health care system as they lack the resources and have pushed back in implementing enhancements due to cost. Unless they are able to find a way to receive funding or are purchased by a large system, smaller sized practices are less likely to implement innovation and join new models. Assistance is available to qualifying small practices through Quality Improvement Organizations and Regional Extension Centers to assist with enhancement and transitions. Unfortunately, there are no upfront financial incentives for providers in MACRA, so providers who are unsure of the long-term financial benefit will be less likely to join innovative models.
In regards to quality measurement and reporting, there are many challenges and drawbacks for providers to overcome to ensure they are achieving high quality standards. As demonstrated in the current Physician Quality Reporting System, providers not achieving quality goals will lose incentive and incur penalties. If providers are unable to fulfill the measures as shown in performance measurement reports, these providers will receive less dollars and be viewed as inefficient and lacking quality. However, factors influencing quality reports may be beyond the control of the individual physician. These reports take months to be generated and may have more to do with the health and demographics of the provider’s population and not necessarily the clinician. If the various measures are deemed necessary to continue participation in the CMS programs, achieving these measures is a must. Developing processes for achieving these measures will initially require additional planning, time and resource investments to ensure participation and protect the bottom line of these providers.
As the push continues towards VBP with an increased focus on measuring performance on quality of care, there are many years of upcoming MACRA rule-making and policy implementation changes ahead. The timeline below discusses the progression of the Quality Payment Program and its associated fees, incentives and payment adjustments. From 2016 – 2019, each year providers will see a 0.5% fee schedule update. Starting in 2019, providers may start the MIPS or APM track, each with its associated payments or penalties. MIPS can be a bonus or penalty starting at 4% and increases to 9% by 2022. APMs qualifying participants will receive 5% bonus payments and be excluded from MIPS adjustments.
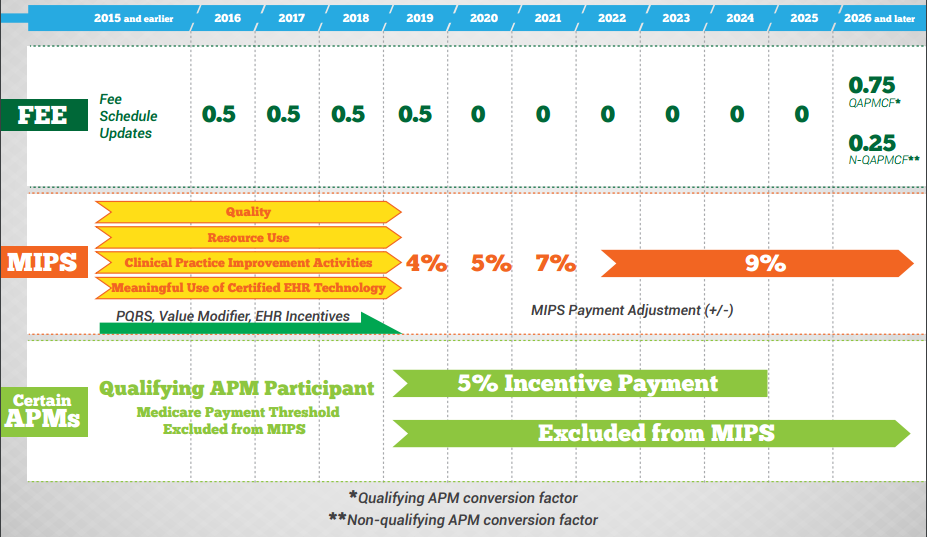
https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/Value-Based-Programs/MACRA-MIPS-and-APMs/Timeline.PDF
Through active integration of quality measures and reporting and participation in APMs will result in an efficient stepping stone to VBP. As CMS rolls out these programs to MSOs and IPAs, this will become a routine part of medical care to improve quality and costs.
About COPE Health Solutions
As health care continues to change, COPE Health Solutions is an expert and remains in the forefront of the industry. COPE Health Solutions is a national mission-driven consulting firm that partners with health systems and payers to develop and implement comprehensive population health management and workforce development strategies. Our history as a student-run homeless family outreach and preventive health community based organization keep us firmly rooted to our commitment to partner only with providers and payers committed to all lines of business, not just focused on profitable Commercial and Medicare lines of business. Today, our nationally recognized team includes experts in the areas of clinical integration, managed care systems design, ambulatory network development, strategic planning, care coordination, health care finance – including value based payment methodologies, Medicaid waivers, Medicare ACOs/demos, provider and health plan contracting and population health. This expertise and our commitment to truly integrate into our client teams has led to long-term client partnerships and many successful implementations. To learn more, contact us at info@copy.laraco.net.